
Welcome to IBJ's “Business Cares: Heart Health Awareness” Microsite
Being aware of symptoms and advocating for yourself can save your life when it comes to matters of the heart. Read the stories of two survivors in this year's “Business Cares: Heart Health Awareness” section. You'll also find informative columns about heart health written by local cardiologists and a calendar of upcoming Heart Health Awareness Month events.
View calendar now View the interactive edition
Students at more than 400 schools in Indiana will begin participating in the American Heart Association's Kids Heart Challenge program. During the program students will get moving with fun activities, learn about keeping their hearts and brains healthy and feel great about helping others. Learn more at heart.org/schools.
On National Wear Red Day, thousands of people, including employees at more than 10,000 companies across the country, will wear red to support the start of American Heart Month. This year is the 24th annual National Wear Red Day. Post a picture of yourself wearing red using the hashtag #IndyGoesRed and tag @AHAIndiana on Facebook, Twitter or Instagram.
7 p.m. / Fishers Event Center, 11000 Stockdale St., Fishers
The American Heart Association will offer free Hands-Only CPR trainings during the Indy Fuel's game against Wheeling.
Congenital heart defects affect nine of every 1,000 births and are one of the leading causes of death for infants less than 1 year of age. Thanks to years of research and medical advancements many congenital heart defects can be fixed.
8:30 a.m. – 12:30 p.m. / Knights of Columbus, 2100 E. 71st St., Indianapolis For information about the breakfast contact Marv Norman at [email protected].
9 a.m. – 3 p.m. / Marion County Clerk, W-122 City County Building, 200 E. Washington St.
The Marion County Clerk's office will conduct wedding ceremonies to raise money for the American Heart Association. Couples who desire a simple civil ceremony or vow renewal can make a $50 contribution to the American Heart Association in lieu of an officiant's fee. Couples can make a reservation by calling (317) 327-5099.
10 a.m. – 2 p.m. / Indiana State Capitol, 200 W. Washington St.
American Heart Association advocates will gather at the Capitol to meet with lawmakers and to learn more about important issues impacting the health of Hoosiers, including Cardiac Emergency Response Plans for schools, creating a statewide stroke registry and more. More information is available at www.midwestregion.quorum.us/event/20269/.
11:30 a.m. ' 1 p.m. / Riverview Health, Noblesville, Entrance 4 and downstairs
Ascension cardiologist Dr. Navneet Lather discusses the latest in heart treatment and care. Lunch provided. For information contact Marv Norman at [email protected].
5 p.m. / Gainbridge Fieldhouse, 125 S. Pennsylvania St.
The American Heart Association and Ascension St.Vincent will offer free Hands-Only CPR trainings during the Indiana Pacers game against the LA Clippers.
10 a.m. – 1 p.m. / Westin Hotel, 241 W. Washington St., Indianapolis
The 21st annual Go Red for Women Experience is the cornerstone event of the Go Red for Women campaign, celebrating achievements in helping women live longer, healthier lives. This year attendees will learn the lifesaving skill of Hands-Only CPR while hearing from heart disease survivors and local leaders. For more information, visit www.heart.org/indygoesred.
5 p.m. / Gainbridge Fieldhouse, 125 S. Pennsylvania St.
Top schools and fundraisers from the American Heart Association's Kids Heart Challenge program will be recognized during the Indiana Pacers game with the Brooklyn Nets. Tickets are available at https://pacers.formstack.com/forms/aha322.
Stroke at 41 leads Indy man to give back
Content provided by Community Health Network
Life can change in a heartbeat, they say. It certainly did for Nick Schellinger, the director of business development at Garmong Construction.
In November 2023, the then 41-year-old was picking up his twin sons from daycare when he started experiencing numbness on the right side of his body. As the numbness spread, he knew he needed to get to the hospital.
“I knew what was happening and was scared,” Schellinger recalled. “I quickly decided to advocate for myself and insisted to the emergency room desk staff that I was having a stroke. All feel-ing from head to toe on the right side of my body was gone. A nurse overheard me and asked me to smile. When it was clear I could not smile, I was taken back into the ER immediately, where I received scans and, soon after, lost the ability to speak.”
Schellinger recognized the “F.A.S.T.” signs of a stroke where:
F stands for face drooping/numbness
A stands for arm weakness/numbness
S stands for slurred speech
T stands for time to get immediate help
Schellinger was treated immediately and, after a week in the hospital, was released with no lasting effects.
“I owe my success story to the fact that I am in construction and have attended countless safety training classes, and I knew what was happen-ing,” Schellinger said. “I knew time was of the essence and I got to a hospital. I demanded to be seen. I knew what to do and advocated for myself. Many in this world do not, and many are not as lucky as I was. I now watch my health more closely and take proper precautions. But my list of action items doesn't stop there. In fact, I believe my story has just begun.”
Schellinger's company participates in the American Heart Association's Hard Hats with Heart program, which provides resources about heart dis-ease, stroke, healthy living and more. As word of his stroke spread, he was soon nominated to participate in the Association's “Leaders of Impact” program, a peer-to-peer fundrais-ing and education program that allows people to give back to the community by supporting the American Heart Association.
Over a seven-week period last fall, Schellinger raised more than $250,000, which was the second-highest total in the country.
“I was honored to be nomi-nated for this program and have the opportunity to make an incredible impact for the AHA, the communities in which we live and those we love and cherish,” Schellinger said.
“We're incredibly proud of Nick's steadfast efforts to help ensure everyone in central Indiana has equitable opportunities for a longer, healthier life,” said Amanda Mills, executive director of the American Heart Association in Indianapolis. “By ensuring access to quality health care and addressing health disparities we are strengthening our collective future, creating a healthier, more vibrant community for generations to come.”♥

New procedure offers hope for atrial fibrillation patients
Content provided by Community Health Network
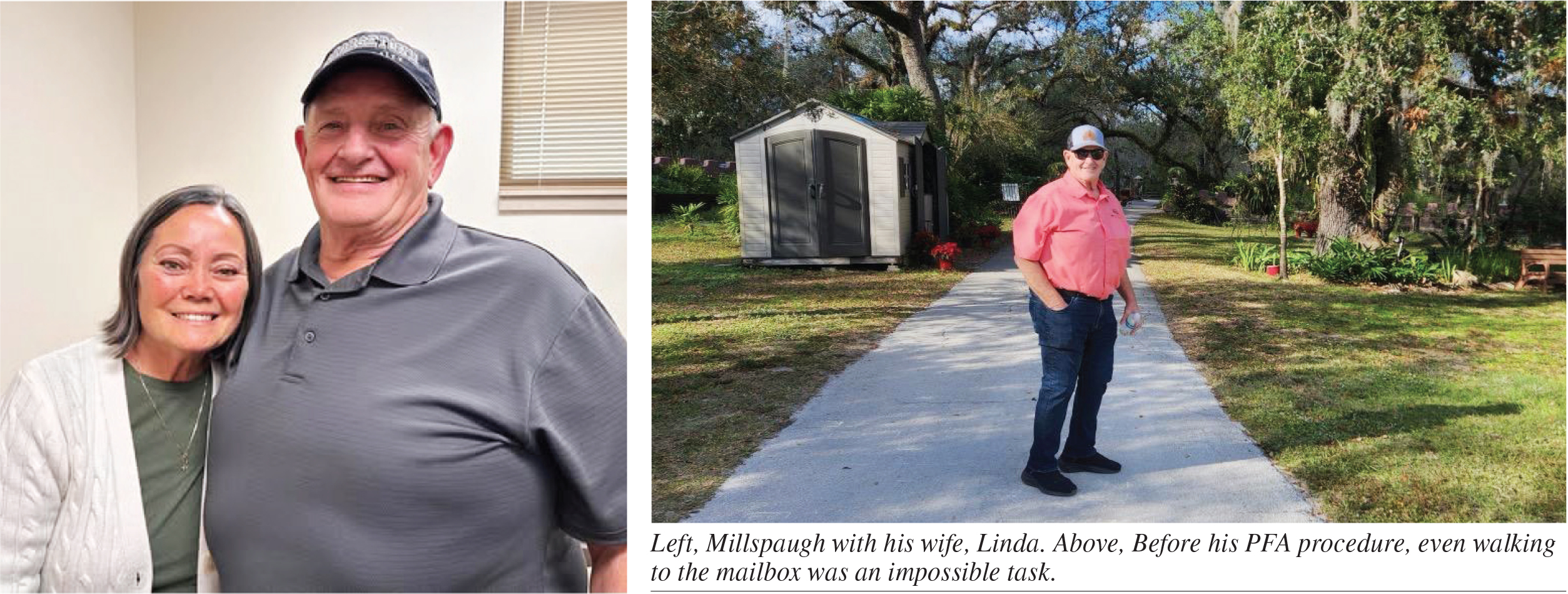
For Rolla Millspaugh, even a simple walk to the mailbox was an impos-sible task. For months, the 68-year-old avoided leaving his North Vernon home, gripped by the fear of having a heart attack.
“It's pretty scary when your heart gets racing, and you don't really know what's going on with it,” Millspaugh said.
Two years ago, Millspaugh was diag-nosed with atrial fibrillation, or AFib, a heart rhythm disorder that impacts millions of Americans. According to the Centers for Disease Control and Prevention, AFib is the leading cause of stroke, contributing to about 158,000 deaths annually. By 2030, more than 12 million people are expected to live with this condition.
For Millspaugh, AFib caused episodes of an erratic heart rate that sometimes exceeded 230 beats per minute. These episodes, lasting days or even months, left him physically and emotionally drained.
“It just felt like you were going to explode,” he said.
Despite trying various medications and undergoing procedures designed to regulate his heart rate, on June 28, 2024, an episode woke him up in the middle of the night, sending him to his local hospital and prompting him to seek a better solution.
Determined to regain control of his health, Millspaugh began researching other options. He learned about a new procedure called pulsed field ablation, or PFA, which had recently received approval from the Food and Drug Administration.
Unlike traditional ablation, which uses thermal energy to create scar tissue and can sometimes damage surround-ing tissue, PFA uses short bursts of high-energy electrical fields to treat AFib. The procedure is not only safer but also faster and more effective.
“People feel better after the proce-dure compared to traditional ablation,” explained Dr. Kevin Trulock, an elec-trophysiologist at Community Heart and Vascular Hospital in Indianapolis. “They recover faster, and most patients can go home the same day instead of staying overnight for observation.”
PFA's efficiency also allows hospitals to treat more patients, a key advantage as the number of people with AFib continues to rise.
Community Health Network, based in central Indiana, was the first health system in the state, and one of the first 10 in the country, to offer PFA. The network has been a pioneer in heart care, introducing several innovative technologies, including the WATCH-MAN device to reduce stroke risk and an extravascular defibrillator to treat sudden cardiac arrest.
For Millspaugh, the opportunity to undergo the groundbreaking proce-dure without leaving Indiana was life changing.
In August 2024, he underwent PFA at Community Heart and Vascular Hospital. Within weeks, he noticed a significant difference.
“Until they did this, I couldn't even get up and go to the mailbox,” he said.
Though PFA is not a cure for AFib, it can dramatically reduce symptoms and improve a patient's confidence in managing their condition, Trulock explained.
“It's not a cure, and some patients may need additional care beyond abla-tion,” Trulock said. “But in Rolla's case, the procedure has given him a renewed sense of confidence in his health, which is a key component to his overall well-being.”
For Millspaugh, the procedure has opened doors to a life he once thought was out of reach.
Since recovering from PFA, he has played golf for the first time in 20 years, attended his grandson's basketball games, and is planning a motor home trip out West with his wife.
Millspaugh said he is grateful for the care he received at Community and credits the procedure with giving him his life back.
“I can't say enough about this and the care I received at Community,” he said.
His primary goal in pursuing PFA was to live without the constant fear that AFib episodes would disrupt his plans. Now, he feels that goal has been achieved.
For the millions of Americans living with AFib, Millspaugh's story high-lights the promise of new treatments like PFA. With the condition expected to become even more common in the coming years, advancements like these offer hope for a better quality of life and a brighter future.
To learn more about Pulsed Field Ablation at Community Health Net-work, visit eCommunity.com/heart.♥
Weight loss and beyond
Fighting heart disease and more with GLP-1 meds
By Tony Bashall
In just five years, experts predict that 50 percent of Hoosiers will be obese. Indiana already ranks among the 10 states with the highest obesity rates in the country. You could say that obesity has become “normal” in the United States.

Yet this “normalcy” is incredibly risky. With a Body Mass Index of 30 or more, a person's chance of having a heart attack, stroke and diabetes Bashall increases four to five times. With a BMI of 35, a person's risk increases 12 times.
Between 1999 and 2020, cardio-vascular deaths tied to obesity have tripled, despite public health experts bringing attention to—and suggest-ing solutions for—the issue. So, what does this mean? It means what we're doing to manage weight isn't work-ing. Many physicians stick with the old formula, “eat less, exercise more.” I've heard that myself as a patient, and I didn't find it helpful. Society tells us you'll lose weight if you wear this activity-tracking device, use this app to track calories, and sign up for our program. Yet we still struggle to make and maintain the appropriate lifestyle changes we must make to shed the weight we think we need to lose and keep it off over time.
This is no doubt why the use of glucagon-like peptide (GLP-1) drugs for weight loss has attracted so much attention. First created to help man-age type 2 diabetes, GLP-1 drugs like Ozempic, Wegovy and Mounjaro have been shown to not only impact weight but also contribute to better heart health, easing of joint pain, and improved liver function.
Simply put, these GLP-1 drugs change the messages between the stomach and the brain. We have natu-rally occurring GLP receptors in our body that help to tell us when we're full after eating. These drugs mimic that action, but with the advantage of lasting for days instead of a couple minutes, sending the signal that “I don't need to eat.” As a result, most patients eat less, are able to maintain a more healthy diet, and lose weight. Many patients will lose between 10 to 25 percent of their body weight.
And this is enough to make a tremen-dous difference in a patient's health. At a 5 percent weight loss, we start to see benefits. At 10 percent, the risk of diabetes is lowered. At 15 percent, the risk of other diseases, including heart disease, can be reversed.
It has become clear that the benefits of GLP-1 medications don't stop at helping to lose weight and managing type 2 diabetes. They can also:
- lower inflammation
- reduce the risk of heart disease and stroke
- stop the progression of some kidney diseases
- reverse fatty liver conditions
- reduce joint pain and ease the symptoms of osteoarthritis
- contribute to better sleep, pos-sibly reducing the need for CPAP machines
- improve function for patients with heart failure and reduce hospital admissions
Someone recently asked me, Dr. Bashall, as a cardiologist why are you interested in these medications? Profes-sionally and personally, I know the toll obesity has on one's health. Yet I also know what even modest weight loss can do. For instance, one patient of mine was taking multiple medications and insulin shots for diabetes. I prescribed one of the GLP-1 injectable drugs, along with a couple of other medications. The result: This patient now doesn't need insulin or many of the previously prescribed meds, and the patient's A1-C level has never been better. With better diabetes control and modest weight loss, this patient's risk of cardiovascular disease has plummeted.
Another patient, an octogenarian with heart failure and a long list of medications, was considering hospice care. We started treatment that included an injectable GLP-1. At a recent follow-up appointment, I admit I didn't recognize the patient at first. The patient had lost 50 pounds, no longer needed a wheelchair, and announced “I feel better now than when I was 60.” We were also able to eliminate at least half of the patients' previous medications.
Clearly, GLP-1 medications have proven to be excellent tools in helping patients achieve better overall health. Medical oversight can help deter-mine appropriate dosages over time and monitor side effects, which are minimal. Combined with the tradi-tional approaches of lifestyle changes, improved diet and increased activity, GLP-1 meds can help improve the well-being of patients and reduce and even eliminate the risks of several diseases, including heart disease.♥
Bashall is a cardiologist practicing at Franciscan Physician Network Indiana Heart Physicians Indianapolis and is director of cardiovascular and cardio-metabolic care at Major Hospital Part-ners in Shelbyville.
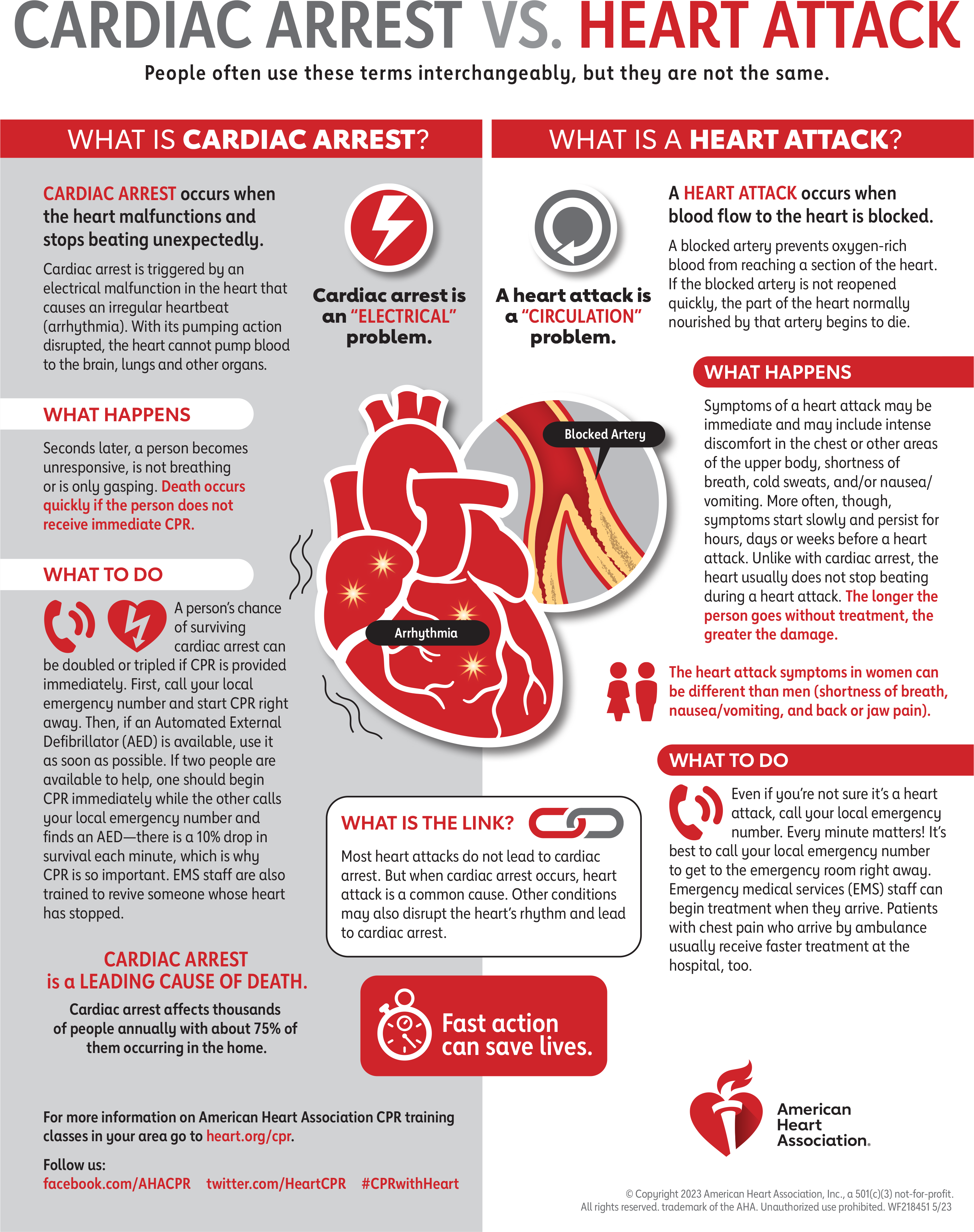
Cardiac Arrest vs. Heart Attack
What you should know about peripheral arterial disease
By Sai Krishna Devarapalli
Peripheral arterial disease, or PAD, is a significant health issue that grows worse each day. And even though it is the third leading cause of atheroscle-rotic-related illness following coronary heart disease and stroke, very few people are aware of it.
PAD is a peripheral vascular disease that affects the arteries outside the heart and brain, Devarapalli such as those in the legs. It is characterized by a buildup of fats, cholesterol, and other substances in and on artery walls, which can cause arteries to narrow, severely limiting blood flow. PAD significantly impacts quality of life, with risks of limb loss and life-threatening events. It is associ-ated with high morbidity and mortality rates.
An estimated 238 million people of all ages are living with PAD worldwide. This is an increase of 20% just in the past decade. Its prevalence is expected to keep growing thanks to key contribu-tors, such as aging populations and lifestyle-related diseases.
PAD rarely occurs in isolation. Tobacco use, diabetes, high cholesterol, and hypertension are major risk factors. When symptoms are present, they can include leg cramps, pain, and poor wound healing. However, most patients experience few to no symptoms, which leads to common misdiagnoses of arthritis and muscle pains.
Diagnosis and Treatment
A PAD diagnosis is made with a simple, noninvasive test called an ankle-brachial index. Anatomical evaluations like angiograms can enhance further diagnosis.
PAD treatment includes revascular-ization (procedures that restore blood flow), and medical therapies aimed at preventing the disease from progress-ing. These include aggressive lipid-lowering therapies, blood thinners, and anti-inflammatory therapies targeted to treat inflammation, which promotes atherosclerosis. About half of patients with symptomatic PAD require lower-extremity revascularization. Severe cases may result in limb amputation.
Our options for treating PAD are growing as our understanding of the disease evolves. In the past few years, many new therapies have emerged, including advances in atherectomy, laser, ultrasonic lithotripsy, drug-coated balloons and stents, and absorbable scaffolds.
Patients with PAD need treatment plans that are customized to their specific needs in order to experience the most optimal outcomes for both life and limbs. Most of these patients have coexisting cardiovascular and cerebrovascular disease, so it is essential to place them on preventive therapies. In addition, supervised exercise offered through cardiac rehab programs can improve walking distance and quality of life.
Need for Public Awareness
PAD's impact is vastly underesti-mated. The rising prevalence of diabetes and obesity is directly correlated to the increase in PAD incidents. As PAD diagnoses increase, so do strokes, heart attacks, limb amputations, and revascu-larization procedures.
As incidents of PAD rise, so should education on what it is. Public health campaigns promoting awareness of coronary heart disease and stroke have played a crucial role in improving survival rates and promoting healthier lifestyles. Similar efforts to raise aware-ness of PAD could reduce this disease's significant impact on our society's health and lead to better approaches to care that will increase a patient's quality of life.
Take Action Now
In the meantime, everyone can take action to prevent PAD. Eat a nutritious diet. Make sure you get some physical activity every day. If you currently use tobacco, stop. In addition, knowing and understanding key heart numbers—blood pressure, cholesterol, and heart rate, along with your family history—allows you and your health care team to determine your risk for developing heart disease, stroke, and peripheral artery disease.
Remember, even if you aren't expe-riencing any symptoms, you may not notice any warning signs until the dis-ease has progressed to a severe stage. By keeping track of your numbers between health care visits, you will be better able to manage your health.
Learn more about heart and vascular screenings and services at Hendricks. org/heart.♥
Devarapalli is a board-certified inter-ventional cardiologist for Community Physician Network Heart & Vascular Care at Hendricks Regional Health Dan-ville and Brownsburg hospitals.
Acknowledging the heart-kidney connection is key to effective care
By Morgan Marcuccilli
Heart disease is the leading cause of death in the United States and Indiana, but Medicare data shows that more than 60 percent of heart failure patients also suffer from chronic kidney disease. Patients with both heart failure and chronic kidney disease are among the highest-risk patient populations at IU Health for both hospital readmission and mortality. In 2019, the American Heart Association formally recognized the link between kidneys and heart failure. This important recognition accelerated the process of building a bridge to connect nephrology (the branch of medicine treating kidneys) and cardiology.
The intertwining of these dis-eases led IU Health to establish a multi-disciplinary clinic between the nephrology and cardiology depart-ments called the Nephro-Cardiology Clinic in July of 2024. The goal is to gain a deeper understanding of the links between these two organs. There are fewer than 15 specialized clinics of this type in the United States.

As a nephrologist at IU Health, I founded the clinic with support from my division at Indiana University School of Medicine. But I also have a long-held interest in cardiology. I was a Riley “kid” and underwent open-heart surgery at the age of three. I'm enthusiastic about this collaboration and the opportunity to provide the highest quality care for patients with heart failure and kidney disease.
The need for specialized clinics catering to patients with complex conditions is becoming increasingly important as patients grapple with the fallout from metabolic conditions such as diabetes and obesity, which are major risk factors for kidney and heart disease. This collaborative approach prioritizes communication between the heart and kidney subspe-cialists and allows the opportunity to create individualized plans for each patient through a team-based effort.
One of the most frequent questions I receive from patients is, “Aren't you talking to my other doctors?” The fact is that physicians often do not share the same electronic medical record or a patient has not signed a consent to release their information to another health care network. With cardiolo-gists and nephrologists working in the same location, the clinic facilitates a connected care plan that is tailored to each patient's unique needs. This approach aligns with the goals of IU Health, which is moving away from a one-size-fits-all approach.
In addition, the clinic leverages advanced technologies, such as bedside ultrasound and the latest research on new medications—including sodium-glucose cotransporter 2 inhibitors and mineral corticoid receptor antagonists—to improve patient outcomes. Point-of-care ultra-sound allows us to assess a patient's volume status in real-time without having to order a formal echocardio-gram or renal ultrasound. It is becom-ing ‘the new stethoscope’ or what is considered to be the future of bedside clinical medicine.
Beyond advanced diagnostics, the Nephro-Cardiology Clinic empha-sizes a holistic approach to health, encompassing medication manage-ment, dietary modifications, and lifestyle counseling. It also promotes patient involvement and autonomy, noting that the most successful patients are those willing to actively participate in meeting their health care goals. The aim is to optimize both kidney and heart function, enhancing patient quality of life, and ultimately reduce health care costs through preventive care.
Currently, patients are referred to the Nephro-Cardiology Clinic through their cardiologist or nephrol-ogist. After being released from the hospital, patients have dedicated nurse navigators who coordinate care plans and check in post-hospitaliza-tion. In the outpatient setting, the Nephro-Cardiology Clinic works in tandem with the Heart Failure team led by Dr. Roopa Rao to ensure dif-ferent medications for the heart and kidneys are not adversely affecting each other to cause electrolyte abnor-malities or other side effects.
The launch of the Nephro-Cardiology Clinic at IU Health is a signifi-cant milestone in the commitment to improve the health of Hoosiers. By providing integrated care for patients with heart failure and kidney disease, the clinic is tackling a major public health issue head-on. Our hope is that we can spread the word about this unique opportunity and keep growing. As we look to the future, it's clear that this integrated, patient-centered approach will be a key driver in improving health outcomes and quality of life for millions of patients worldwide.♥
Marcuccilli is a nephrologist at IU Health.