Subscriber Benefit
As a subscriber you can listen to articles at work, in the car, or while you work out. Subscribe Now
Lawmakers are holding their collective breath in anticipation of Dec. 17 forecasts for tax receipts and Medicaid needs that will determine how they’ll proceed with writing the state’s next two-year budget and funding priorities like education.
If the revenue forecast is dismal and the projections for Medicaid spending are high, lawmakers could face tough decisions as they try to pass a balanced budget.
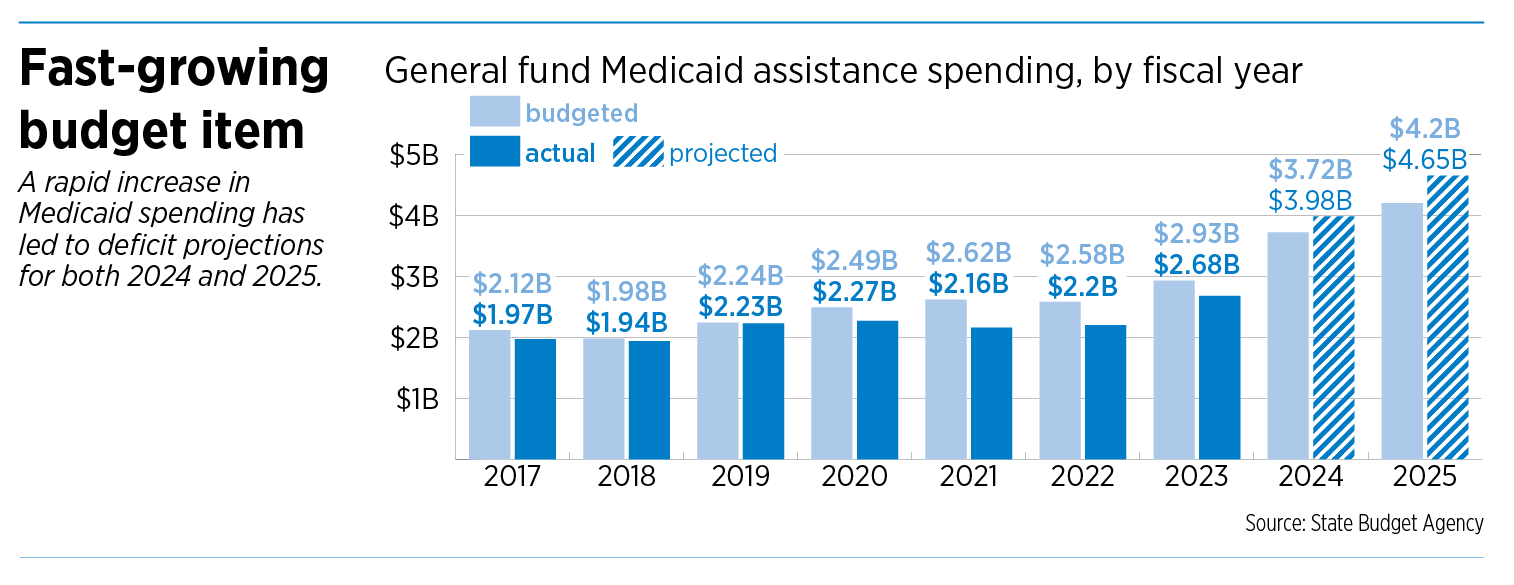
Neither would be a surprise. For the past three months, state revenue has underperformed estimates released a year ago. And last December, lawmakers learned about a $985 million shortfall in the state’s Medicaid budget.
That’s in part why Medicaid—the second-largest recipient of state funding behind K-12 education—remains one of the next budget’s biggest questions. And Indiana isn’t alone. Across the country, states are navigating the program’s surging costs.

“I’m very concerned about Medicaid,” Senate Appropriations Chair Ryan Mishler, R-Mishawaka, told IBJ. “That is my number one concern right now.”
On Friday, Gov.-elect Mike Braun told reporters that he does not want to cut Medicaid access in order to reduce surging costs. Rather, the Republican said he is focused on “lower hanging fruit,” such as reducing Medicaid fraud.
Putting pressure on hospitals and insurance companies through competition and transparency will also lower costs, he said.
“Health care in general is not going to get any easier until we start bringing the costs of health care down,” he said. “That’s insurance companies and hospitals.”
State officials blamed the fiscal year 2024 shortfall on forecasting errors that underestimated the enrollment in and use of Medicaid, which pays for health care primarily for low-income people and those with disabilities.
Medicaid enrollment grew significantly during the pandemic when the federal government blocked states from kicking users off the program, even if they no longer met eligibility guidelines, and incentivized states to expand the program by paying for a larger share of it. Once that temporary funding ended, Indiana—and other states—rolled back the expansions, but they found that more residents remained eligible than expected.
Experts are still digging into why that is and why costs are growing so sharply. But they’ll need to come up with answers quickly.
The General Assembly will reconvene on Jan. 8 to begin official business, including building the 2026-2027 budget—which will take effect July 1, the beginning of Indiana’s 2026 fiscal year. Lawmakers will need to send the governor a budget bill before state law requires them to adjourn in April or they’ll face a special session to finish the work. The fiscal 2024-2025 budget totaled $44.5 billion.
Federal/state program
Lawmakers have limited choices when it comes to Medicaid. They can account for the increasing costs by boosting the share of the state budget dedicated to the program, pull back on the few optional services Indiana offers, cut reimbursement rates to providers, try to cut administrative costs and fraud or do some combination of those.
Medicaid is largely funded by the federal government, which has traditionally paid about two-thirds of the cost of services, with states picking up the remainder of the tab. The federal share increased to as much as 90% during the pandemic; in Indiana, that share dropped to about 75% in fiscal year 2023.

In Indiana, the Family and Social Services Administration administers Medicaid in accordance with federal guidelines, which include both required and optional services. For example, inpatient and outpatient hospital services and home health care are federally required to be covered, while dentures, eye care and physical therapy are optional.
The state also sets eligibility guidelines and determines how much care providers are paid, which means both categories offer potential for savings. But state officials have so far been mum about what changes they’ll seek in the new budget.
“The focus will be on trying to just get control of the program, cut where we can, be more efficient where we can,” Republican Sen. Travis Holdman of Markle told IBJ. “We just have so many dollars to spend and a budget to live within, so we’ll have to just do our best.”
Shortly after state officials revealed the shortfall in the Medicaid program, FSSA announced several cost-cutting measures, which were projected to save $300 million. That included changes to an attendant care program that meant parents who act as caregivers for medically complex children would be paid a per diem instead of an hourly rate as they had been. The change sparked outrage among the program’s users, offering a preview of what’s to come for lawmakers if they consider significant changes in programs or eligibility.
So far, lawmakers and state officials have offered few details, saying much of their decision-making will depend on the upcoming forecasts. Usually, the revenue forecast guides the budget, Mishler said, but this year, the Medicaid forecast will have a more significant impact.
“I’m anxious to see what this December forecast is going to look like,” Holdman said. “After that, I think we’ll have a little better idea where we’re headed and [what it’s] going to look like for us.”
Cris Johnston, director of the Office of Management and Budget, told IBJ it would be premature to speak about how Republican Gov. Eric Holcomb’s administration is preparing for the next budget before the Dec. 17 forecasts. And Holcomb will leave office Jan. 13 when Braun is sworn in.
State of the budget
Across the country, states are experiencing a slowdown in sales and income tax growth, said Brian Sigritz, director of state fiscal studies for the National Association of State Budget Officers. That will lead to more difficult budget negotiations in legislatures in 2025.
Still, many states—including Indiana—are in a fairly good position to adjust, in part because they used increased tax collections during the pandemic to build up reserves or pay down debt, Sigritz said.
But rising Medicaid costs are a complication. And no state is a shining example for others to follow, Sigritz said, because every state is dealing with post-pandemic changes in their programs.

Stephanie Wells, president of the Indiana Fiscal Policy Institute, which tracks budget negotiations, said fiscal leaders warn every year that the budget is tight. “But I believe them this year,” Wells said. “I don’t think there’s going to be a lot of new spend on anything.”
Statehouse leaders have emphasized their focus for 2025 is on passing a budget that is balanced, meaning it doesn’t spend more than the state is expected to receive in revenue.
But Senate President Pro Tem Rodric Bray, R-Martinsville, said during the Legislature’s Organization Day on Nov. 19 that Medicaid is an issue that “threatens to take over the budget.” The day before, House Speaker Todd Huston, R-Fishers, said on a panel that cutbacks in other areas might be required to ensure the state can pay its Medicaid bills.
“Whatever the forecast says we need to invest in Medicaid, we’ll invest in Medicaid,” Huston told reporters Nov. 18. “It’ll just mean that we have to make larger investments in Medicaid. We’ll have to make smaller investments in other things.”
But those projections are difficult, Sigritz said, because of the work states are doing to unwind the pandemic-era Medicaid provisions and funding increases. In the process, many states are discovering that more high-cost individuals with serious or long-term health conditions are now eligible for Medicaid than before the pandemic, he said.
Waiting to learn how much the state needs to spend on Medicaid has left the future uncertain for proposals like a Republican-backed plan to provide vouchers to all Indiana students who want to go to private school, regardless of family income. In addition, Braun plans to advocate for property tax cuts, which reduce revenue to local governments. Typically, lawmakers look to replace that local government revenue, which could be tricky if the budget is tight.
Holdman, the Senate’s majority leader and chair of the Senate Tax & Fiscal Policy Committee, told IBJ that Medicaid accounted for less than 10% of the state budget when he was first elected to the Senate in 2008. It now sits at about 17%.
Mishler said Medicaid will likely make up 17% to 20% of next year’s spending plan. His goal is to limit the growth in Medicaid spending to $200 million a year, though he acknowledged annual growth might be closer to $400 million.
“The rate of the increase in Medicaid is greater than our overall revenue increase,” he said. “You can’t sustain that kind of growth.”
Mishler said that growth is unlikely to be fixed in a single legislative session. The problem took time to build, he said, and will take time to solve.
And Sigritz said that even after states work through post-pandemic complications, Medicaid costs are likely to continue to grow as health care costs grow.
“It’s a long-term fix, but we have to get on it this year,” Mishler said. “I think we will see that it’s not going to stop growing, but my goal is to slow the increase of the growth … . It’s just increasing too fast, and we need to slow that level down.”
Overwhelming enrollment
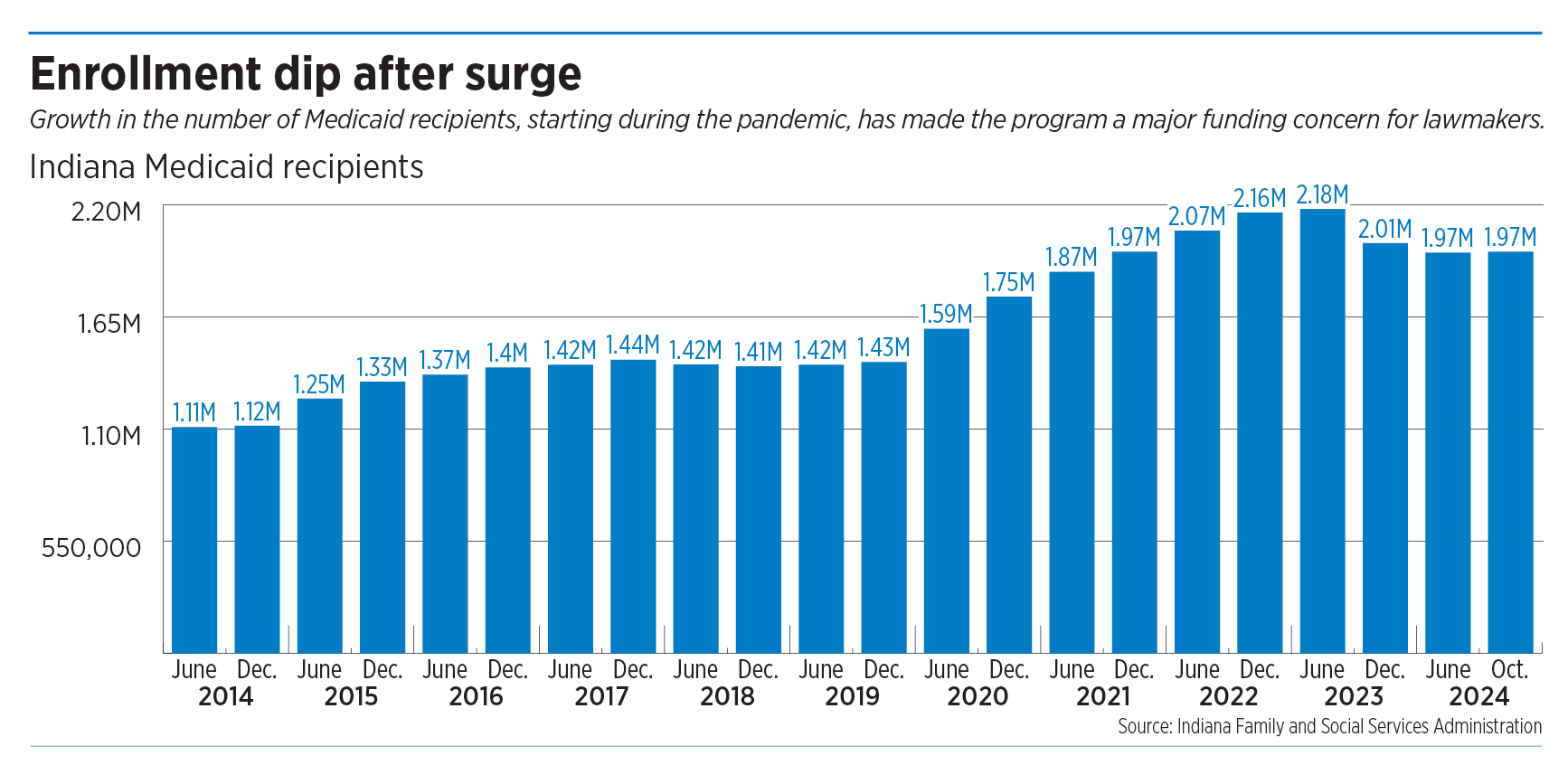
Over the past decade, enrollment in Indiana’s Medicaid program has increased about 80%, peaking in May 2023 at 2.23 million. FSSA counted 1.97 million enrollees in its October 2024 report.
Indiana began the post-pandemic job of removing ineligible Hoosiers from Medicaid in May 2023—a process that officials expected would drop enrollment by some 400,000 by May 2024. Instead, enrollment fell by only about 250,000 people and has remained at about the same level since.
Wells, of the Indiana Fiscal Policy Institute, said those numbers indicate Indiana’s Medicaid problem isn’t just a fiscal issue. It’s a “human issue,” she said.
She said state agencies and lawmakers need to dig into the causes of enrollment growth, which she said was on the rise long before the pandemic. “Framing this just as a budgetary issue is sort of missing the point, which is that more and more Hoosiers are needing these programs,” she said.
And Wells said the state’s aging population—which is more likely to have chronic conditions and require long-term care—will complicate future Medicaid spending. FSSA estimates that nearly 19% of the state’s population will be over the age of 65 by 2025, and the fastest-growing age demographic is those over 85. Medicaid and Medicare, which is available to everyone at age 65, are the biggest payers of long-term-care costs.
To try to control Medicaid costs, FSSA in July launched its fourth managed care program, called Indiana PathWays for Aging. State leaders believe the program could save the state money by paying a managed-care provider a flat fee for services for older Medicaid recipients, rather than paying per service. The goal is to incentivize the managed care provider to make efficient choices.

Kim Dodson, CEO of the Arc of Indiana, which represents children with intellectual and developmental disabilities, said the pandemic created other problems—including those related to mental health and unhealthy lifestyles—that could be increasing Medicaid costs.
Altogether, she said, it has been a “perfect tsunami” for a state already struggling with its public health.
“At some point, we should know that the unhealthiness of our population in Indiana is going to catch up with this,” Dodson said. “We’ve got to do more to prevent some of these chronic conditions, rather than just pay for them after they happen.”
Moving forward
In an agenda released this week, Braun listed a “balanced budget that addresses the state’s deficit while reforming Medicaid spending” as a key priority.
He said during his campaign that he hoped to reduce costs in part by requiring Medicaid enrollees to visit their primary care physician before an emergency room in non-emergencies and allowing Medicaid to reimburse providers who collaborate on a treatment plan rather than referring patients to another facility.
He also said he would seek to root out any mismanagement or fraud within the state’s system with a Medicaid audit and expanded authority for the attorney general’s fraud team. On Friday, Braun called the amount of fraud in Medicaid “astounding.”
FSSA, which will be under new leadership after Braun takes office, told it would address IBJ’s questions about Medicaid at the forecast on Dec. 17.
Legislative leaders, meanwhile, are looking for answers.
Mishler said he’ll be looking at whether to make changes in eligibility requirements and long-term-care services. He said, for example, that wealthy people can move around their assets to qualify for Medicaid.
Mishler also suggested that FSSA should be led by a secretary with a financial background rather than one with a health care or social service background, which has traditionally been the case.
House Minority Leader Phil GiaQuinta, D-Fort Wayne, said the Medicaid program needs more transparency and better data reporting, so everyone in state government is on the same page. That would help lawmakers develop better policy without indirectly affecting “our most vulnerable Hoosiers,” he said.
“We can fix this, and it needs to be fixed,” GiaQuinta said.
And he suggested that spending money on Medicaid services should be prioritized over some GOP agenda items, such as private school vouchers.
Dodson said any changes should be done after a thorough vetting. She’s worried the legislative debate will turn into a Whac-a-Mole game as lawmakers look for places to cut.
She said a better focus would be pressuring hospitals and insurance companies to lower health care costs and increase coverage. She also said the state needs to spend more on preventive health care.
“A lot of this takes time, and I’m not convinced that we’ll be able to have extremely thoughtful conversations within four months in a fast-paced session,” Dodson said. “We need to force ourselves to, again, not make knee-jerk reactions and to be thoughtful about some of these cuts, because I think the consequences of some of them could be really harmful to us long term.”•
Please enable JavaScript to view this content.
The federal government paid Indiana $17.9B for Medicaid expenses based on eligibility. The issue arises when the State legislature takes monies from that pot (roughly $700M), moves it to the general fund, and then acts Pikachu face in surprise when there is a deficit. Boils down to poor leadership.
There is a simple fix – stop cutting taxes and generating taxpayer refunds on the backs of the elderly and the medically complex.
So simple no one will talk about it… because they need for it to not be on the table as an option. We are a very pro-life state as long as it doesn’t cost us a cent. Then, the interest goes away.
What about the surplus savings from the previous 5-6 years where the budgeted amount was more than the actual spend?
If we actually ran our government like a business, or any financially responsible household, we would’ve saved some of that excess money, figuring that at some point in the future, there would be years in which expenses outpaced income.
We passed laws to make that situation trigger automatic taxpayer refunds, because it’s fiscally irresponsible for the government to save too much for a rainy day.
But the best part? We have a rainy day fund, a surplus that our legislators love to brag about. But when a rainy day comes and we might need to tap those funds because they made a big forecasting error? We instead choose to slash spending on people with disabilities.
And as mentioned by someone else, that’s on top of all the federal money intended for the care of the elderly that we are instead diverting to hospital CEO salaries and big fancy new hospital buildings while the elderly rot away in abysmal, understaffed nursing homes.
I mean, to me, when I explain it that way, it makes us sound like a cruel bunch of folks. I guess I don’t understand why others aren’t outraged about it.
“Over the past decade, enrollment in Indiana’s Medicaid program has increased about 80%”. Over time Medicaid will include all but the 1%. Shortly, it will be the top spend in the state budget, just like the trend of social programs at the national level. It’s a bit like going to the grocery store and seeing all the healthy people parking in the Handicapped spaces with a disabled tag on their car.
Indiana is not a pro-life state. It’s a pro-birth state. What happens to you and your child after birth is all part of God’s Plan, not a part of the state budget….
I’m generally pretty amused when legislators decide the best way to rein in Medicaid is to cut reimbursement to hospitals, doctors, and other providers, then complain about increased costs in the insured market. Or the lack of providers willing to provide services for medicaid recipients. If you cut my compensation, I’m less likely to do your lower paying work. Or, I charge my other patients more so the average per patient reimbursement rate stays approximately the same. Those other patients probably have private health insurance or VA or Medicare, and so those costs go up. That way I can keep paying my staff and paying for my office facilities.
Just go tell the doctors their incomes are going to be lower…see how that works for you. See if the doctors and other providers stay in Indiana to provide their services.