Subscriber Benefit
As a subscriber you can listen to articles at work, in the car, or while you work out. Subscribe NowAfter working for three months straight at Detroit Medical Center, Said El Zein noticed that the coronavirus patients who began arriving in May appeared less sick than those who came before.
More than 4,000 miles away in northern Italy, researcher Chiara Piubelli was struck by the same thing.
Rafael Cantón, an infectious-disease specialist in Madrid, also marveled at the change. “It’s totally different,” he said last month of the falling admissions at his medical center, noting that only 130 of 1,000 beds were full despite surging infections—a huge change from early spring when every bed was occupied.
Death rates from the novel coronavirus are lower in hot spots around the world, even as new infections accelerate in what may be the pandemic’s next wave. Scientists are confident the change is real, but the reasons for it—and whether it will last—are a matter of intense debate.
“Is this a trend or a blip?” asked Joshua Barocas, an infectious-disease specialist at the Boston University School of Medicine. “Nobody really knows.”
 The mortality rate of the coronavirus has been a moving target since the outbreak began.
The mortality rate of the coronavirus has been a moving target since the outbreak began.
Early reports out of China put it as high as 7%. But that was based mostly on hospitalized patients, and by the time the wave hit the United States, epidemiologists believed it was closer to 2 to 3%. Now, factoring in asymptomatic infections, as well as mild cases that might not be part of official tallies, the Centers for Disease Control and Prevention puts the mortality rate at 0.65%.
Barocas emphasized that even the lowest estimates represent the potential for millions more deaths. The United States already has the highest number of cases in the world and the most recorded deaths of any country. Though its 330 million people represent roughly 4.25% of the world’s population, the country has recorded just over 20% of deaths from COVID-19, the disease caused by the coronavirus.
As we enter a new phase of the pandemic, Barocas said, with much of the country experiencing colder weather amid a reopening of more workplaces and schools, it’s too soon to be confident that mortality rates won’t tick up alongside case counts, as young people spread the disease to their elders.
He called this time “a cliffhanger moment.”
Public health officials cite multiple reasons for the lower death rates: They note a shift in the demographics of who is being stricken with the virus, with younger people making up the bulk of new infections. More widespread testing is capturing a more diverse range of people and illness, and improved treatment strategies that include antivirals and steroids are saving more lives.
But some researchers speculate there may be more to the story.
One prominent but still unproven theory suggested by early research is that we miscalculated humanity’s susceptibility to the coronavirus, and that a slice of the population may be partially immune, perhaps due to previous exposure to the common cold coronavirus, childhood vaccinations or something else.
The other possibility is that something important has changed in our environment—the weather, behaviors or the virus itself.
Most viruses lose their killing edge eventually, due to a lack of hosts, mutations that make them less deadly, or new treatments or vaccines. The novel coronavirus will, too, experts say, but it’s a matter of when and how many lives are lost until then. But most scientists doubt that’s what we are seeing now, based on genetic sequencing research.
One idea that has generated a lot of discussion recently, bolstered by two back-to-back studies—El Zein’s and another from Italy, presented in late September to the European Society of Clinical Microbiology and Infectious Diseases—is that social distancing and masks are reducing the dose of virus people are receiving, resulting in less-severe illness.
As El Zein and other doctors in Detroit probed why their patients appeared to be less ill, they were startled to find that one indicator in particular changed dramatically over time: viral load.
Among 708 patients treated by early summer, the average viral load—a measure of the particles of virus in the body as measured by nasal swabs—fell almost on a weekly basis. In most infectious diseases, including Ebola, HIV/AIDS and hepatitis, the higher the load, the worse the outcome.
El Zein saw glimmers of hope in the findings: Could it be that the steps being taken to mitigate the coronavirus’s effects were showing success?
Monica Gandhi, an infectious-diseases researcher at the University of California at San Francisco, shares that view. If the initial viral dose—known as the “inoculum”—is lower, she theorized, people’s bodies are able to fight back more effectively.
This “likely indicates an ability to control the viral infection better, and, therefore, have less severe disease,” Gandhi said.
Risk of death
Of the many mysteries of the coronavirus, perhaps the most important to the average person is his or her risk of death. For smallpox, it’s about 10%, thanks to treatments. For Ebola, it’s about 50%. For rabies, it’s almost 100%, making it the most lethal infectious disease on the planet.
President Donald Trump has repeatedly talked about coronavirus mortality rates, even claiming on Fox News in July that the United States had the “number-one low-mortality rate.” Those claims are incorrect, according to the White House’s own data (fact-checkers pointed out that the chart he was looking at that day was upside down). But the confusion underscores how complex the subject is and how such rates can vary dramatically over time, country, region, age and other factors.
“What you are seeing is a misapplication of data and statistics that ends up being overtly false and sometimes very, very misleading,” explained Amesh Adalja, a senior scholar at the Johns Hopkins Center for Health Security.
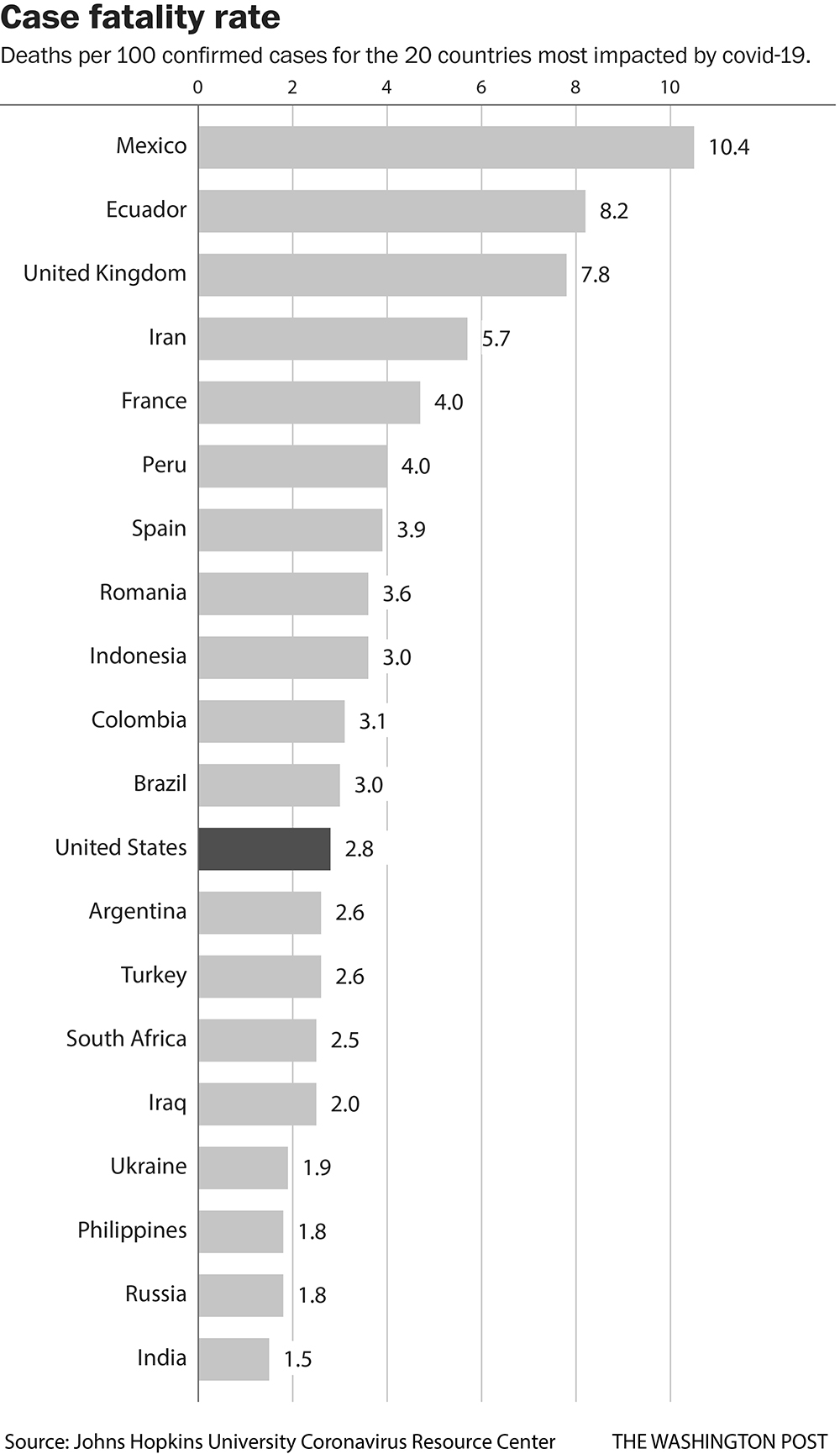
There are many different ways to measure deaths. The most-cited numbers—the ones often released by hospitals—are case fatality rates, or the percentage of deaths among confirmed cases. In contrast, the infection fatality rate is typically an estimate of deaths as a proportion of all those believed to be infected, including people who are asymptomatic or who have mild cases and may not have bothered to get tested, so they would not be counted as part of official tallies. So the former number often looks scarier than the latter.
According to a Johns Hopkins University analysis, which is updated daily, the case fatality rate in the United States was 2.8% as of Thursday. That compares with the CDC’s 0.65% estimated infection fatality rate—which includes confirmed cases plus an estimate of those who may not even know they have been exposed. The case fatality rate in the United States is much higher than in South Korea, Taiwan and Iceland, where it has been below 2%, but lower than in some other hard-hit countries, such as Iran, Brazil, Spain and France.
Some public health officials suggest part of the change in mortality rates is partly a mathematical trick: The more people we test, the larger the denominator of positive cases and the lower the mortality rate.
At the peak of Spain’s epidemic earlier this year, for example, Cantón said, he was doing 500 PCR tests a day, but now it’s more than five times that.
“It looks like we have more positive patients now,” said Cantón. “But this is because we are doing more diagnosis.”
Rinesh Parmar, an intensive care doctor who heads the United Kingdom’s Doctors’ Association, agreed: “The amount in the community was grossly underestimated. We were undertesting.”
Epidemiologists also look closely at deaths per 100,000 people in the population. Because that rate is less dependent on the wild variations in testing capacity, it can be a useful number to compare regions or nations.
To put these numbers into context, the infection fatality rate for the flu, Adalja said, is about 0.1%, making the coronavirus about six times more deadly.
“I think people don’t realize a small percentage of a big number is still a very big number,” he said. Sixty-five hundredths of the U.S. population of roughly 330 million, he pointed out, is 2.145 million—or 2.145 million potential deaths.
Viral loads
The earliest reports of a less-deadly coronavirus came on May 31 and drew widespread skepticism. Alberto Zangrillo, head of the San Raffaele Hospital in Milan in the northern region of Lombardy, which had been the epicenter of Italy’s outbreak, and Matteo Bassetti, from a hospital in Genoa, conjectured that the virus was weakening.
Zangrillo provided the first evidence that viral loads might be linked, stating that in the previous 10 days, nasal swabs taken at his hospital in Milan detected “absolutely infinitesimal” amounts of the virus as compared with the previous two months.
The claims were quickly denounced by public health officials who said there was no evidence of any change in the virus’s lethality. But over time, to some scientists’ surprise, the data has borne out the falling mortality rates and decreased viral load.
An Aug. 13 letter published in JAMA by doctors at Houston Methodist, which operates eight hospitals, reported huge differences between what they called surge 1 and surge 2 patients. In surge 2, which took place from May 16 to July 7, a smaller proportion of patients required intensive care (20%), as compared with those seen earlier, from March 13 to May 15, during surge 1 (38%). They spent less time in the hospital (4.8 days versus 7.1 days).
Most importantly, the later patients were much less likely to die—5.1% versus 12.1%.
A broad analysis of 53 countries and regions with the highest coronavirus death rates identified similar trends. Published in September in Transboundary and Emerging Diseases by a group of American and Chinese researchers, the report found that 80% of countries and regions estimated lower case fatality rates in the disease’s second wave. The paper cited numerous possibilities for what might be driving the shift, including that the most vulnerable had already been infected and died in the first wave. Other theories involved better preparedness, the younger ages of those infected and more favorable environmental conditions, including warmer weather.
“Current evidence remains limited to suggest which of the above hypotheses is more plausible,” the authors wrote. However, they said the classical epidemiological triangle model, which states that “the interactions of the host, pathogen and environment determine the characteristics of outbreaks, rather than one or two factors alone,” likely holds true for the coronavirus.
Viral loads have been one of the most mystifying aspects of the virus.
The now widely available nasal swabs, or PCR tests, give a simple binary yes or no answer about the presence of the virus. But scientists have recently made new discoveries about the importance of the quantity of virus people carry.
When it comes to infectivity, scientists generally believe a negative PCR test, which indicates what is basically a viral load of zero, means you can’t transmit it. This is why the CDC originally recommended two negative tests 72 hours apart before people came out of self-isolation. A high viral load, on the other hand, is believed to mean higher infectivity.
There’s less certainty about how viral load relates to the patient’s own clinical course. Previous studies on influenza tell us that higher viral loads in hospitalized patients are generally not associated with worse outcomes. In contrast, for patients with MERS or SARS—the other severe coronaviruses—higher viral load was an independent risk factor for mortality.
The new Italian viral load study seems to support that link for the novel coronavirus, too. It found that in 373 patients seen in the emergency room in the city of Negrar in northern Italy, viral load declined from March through May, corresponding with a sharp drop in intensive care admissions over those months, down to zero in May.
In a presentation to other scientists in Europe last month, Piubelli, a researcher at Sacro Cuore-Don Calabria Hospital, surmised that “lockdown measures had an impact not only in the absolute number of infected people but also on the severity of clinical manifestations.”
El Zein’s study found more direct evidence that high viral load appears correlated with increased mortality. But the findings are considered preliminary because the team is still analyzing possible confounding factors, such as differing treatments, to see if the relationship holds. In the first week of the study, about 25% of the viral loads were high, half were intermediate and 25% were low. By the fifth week, about 12% had high viral loads, and in the sixth week, no patients had high viral loads.
The death rate of patients in the high viral load group was 45%, compared with 32% of those in the intermediate group and 14% in the low group.
El Zein said the relationship was so striking that he went back to the lab to check, double-check and then triple-check equipment, and to try to figure out whether anything had changed with the procedures for collecting samples, but found no differences.
“It definitely wasn’t by chance or by mistake those numbers are going down,” he said.
One puzzling thing, he noted, is that some studies have shown that children with high viral loads appear to be completely asymptomatic, although those levels correlate with those of adults in intensive care. Separately, the new coronavirus mutation becoming dominant in the world has been associated with higher viral loads in at least one study. El Zein has been stumped about how to reconcile that with his analysis and others of lower viral loads among recent patients.
As cases, hospitalizations and deaths in the United States and Europe have ticked upward in recent weeks—albeit with a lower proportion of deaths than in the past—some health officials have expressed concern that they will be overwhelmed by a slower but more sustained second wave. If the virus spreads back to older people, as many fear is inevitable, death rates may rocket back upward.
Even in Germany, considered a model for coronavirus control and which stood out this spring as an anomaly with a low case fatality rate of less than 0.5%, Health Minister Jens Spahn warned the rate would likely rise. Already, there are 470 patients in intensive care, double the number of a month ago, he said.
“People think that the virus isn’t as serious because we got through the summer well,” he said. “But that’s a false conclusion. It was because we took preventive measures that we did well.”
Spahn blamed the increase on a lax attitude among the younger population that “want to party, to travel, and think of themselves as invulnerable.”
Across the rest of the world, alarmed governments are scrambling to bring back restrictions that haven’t been in place since spring: Paris has closed its bars, Madrid has ordered residents not to leave the city, and Moscow has told companies to make sure at least 30% of their employees are working remotely starting next week.
In New York on Tuesday, about 100 public schools were ordered closed in neighborhoods that have seen a resurgence of the virus.
“It’s a matter of time before we see a rise,” said Steven Van Gucht, the head of viral diseases at Sciensano, Belgium’s national public health institute. “The characteristics of the virus have not changed.”
Please enable JavaScript to view this content.
Public Health Officials call the declining mortality rate due to increased testing a “mathematical trick”. Wow. Virginia, is that you?